



Background
The inflammation of the skin surrounding a fingernail or toenail (referred to as paronychia, or colloquially as a whitlow), is a common skin problem. Paronychia is described as either acute (lasting less than 6 weeks) or chronic (lasting more than 6 weeks) and these groups are thought to have slightly different aetiologies.
Acute paronychia usually occurs secondary to infection or drugs. With infection there is trauma to the skin surrounding the nail, allowing the entry of pathogens (frequently skin flora e.g., Staph. aureus or Strep.pyogenes, however oral flora are also common). Viruses can also cause paronychia, e.g. herpes simplex (herpetic whitlow) or fungi such as candida.
Pre-disposing factors to acute paronychia include:
- Nail biting or picking at surrounding skin
- Sucking of thumbs/fingers
- Manicures
- Ingrown nails
Certain drugs can disrupt the skin barrier and pre-dispose to acute paronychia, such as oral retinoids (isotretinoin). Other drugs include antiretrovirals, BRAF inhibitors (e.g. dabrafenib), cytotoxic chemotherapy drugs (e.g. taxanes) and epidermal growth factor receptor inhibitors (e.g. erlotinib).
The aetiology of chronic paronychia is not completely understood. However it affects people whose skin is repeatedly exposed to wet, cold environments or irritants; for example: domestic workers, farmers, fishermen. It can also occur in those with chronic inflammatory skin disorders, such as atopic dermatitis or psoriasis.
Signs and symptoms
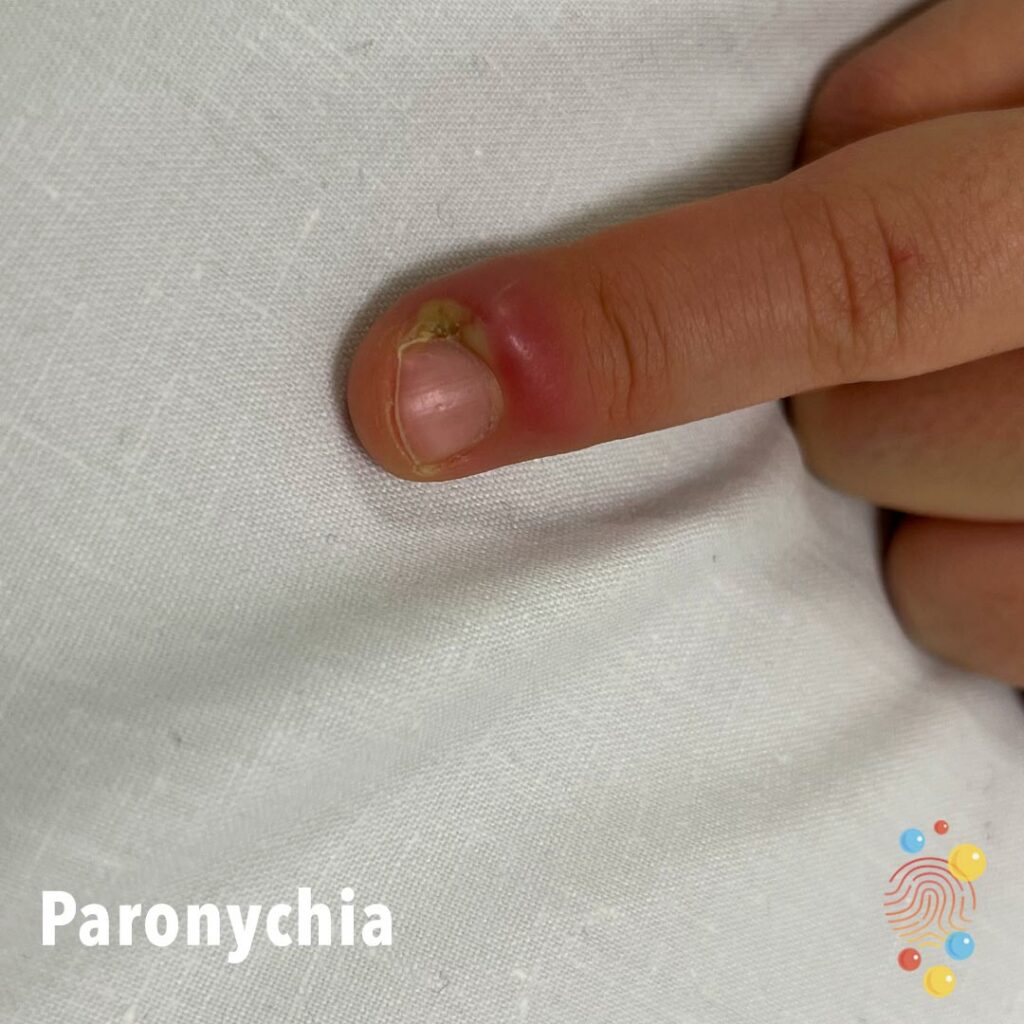
Acute paronychia presents with the rapid onset of pain, swelling and erythema to the nail fold skin, usually within several days of trauma to the area. It generally only affects a single nail fold (however can spread to form a ‘runaround’ paronychia) and may or may not involve abscess formation.
Chronic paronychia has a more indolent presentation, starting with erythema and swelling of the (often proximal) nail fold. It then tends to spread to the lateral nail folds and to other digits. There is loss of the cuticle and these combined changes can allow entry of pathogens into deeper tissues. The nail plate becomes dystrophic, with ridges and discolouration.
Diagnosis
Acute paronychia is a clinical diagnosis based on the signs and symptoms above. Swab and pus samples can be taken to further guide management.
Differential diagnoses:
- Felon
- Acrodermatitis continua of Hallopeau
- Herpetic whitlow
Chronic paronychia diagnosis is also clinical, supported by a history of inflammatory skin disease and/or exposure to irritants.
Management
Acute paronychia management may involve:
- Regular warm water soaks to the affected area
- Topical antiseptics
- Topical or oral antibiotics
- Incision and drainage of any abscess present
Chronic paronychia management includes avoiding any environmental triggers, irritants or allergens. Alternatively, waterproof gloves, and frequent use of barrier creams may help. Any underlying inflammatory skin disease should also be treated (e.g. with topical steroids) and infections treated according to microbiology results.
References
BMJ Best Practice (2020) Paronychia, [https://bestpractice.bmj.com/topics/en-gb/350], accessed 17th October 2022.
Goldstein B., Goldstein A., Tosti A., (2021) Paronychia, UpToDate, [https://www.uptodate.com/contents/paronychia#H2193941350], accessed 17th October 2022.
Oakley A., (1997) Paronychia, DermNet New Zealand, [https://dermnetnz.org/topics/paronychia], accessed 17th October 2022.