
Background
Erythema multiforme is an acute and often relapsing mucocutaneous syndrome that is self-limiting. It is usually mild and related to an acute infection (in 90% of cases), commonly a recurrent herpes simplex virus (HSV) infection. Medications are less common triggers.
EM can occur in patients of any age but is most common in adolescents and young adults. The male-female prevalence of EM is 3:2. It is recurrent in at least 30% of patients. Predisposing genes have been reported including associations with the HLA-DQB1*0301 allele.
Signs and symptoms
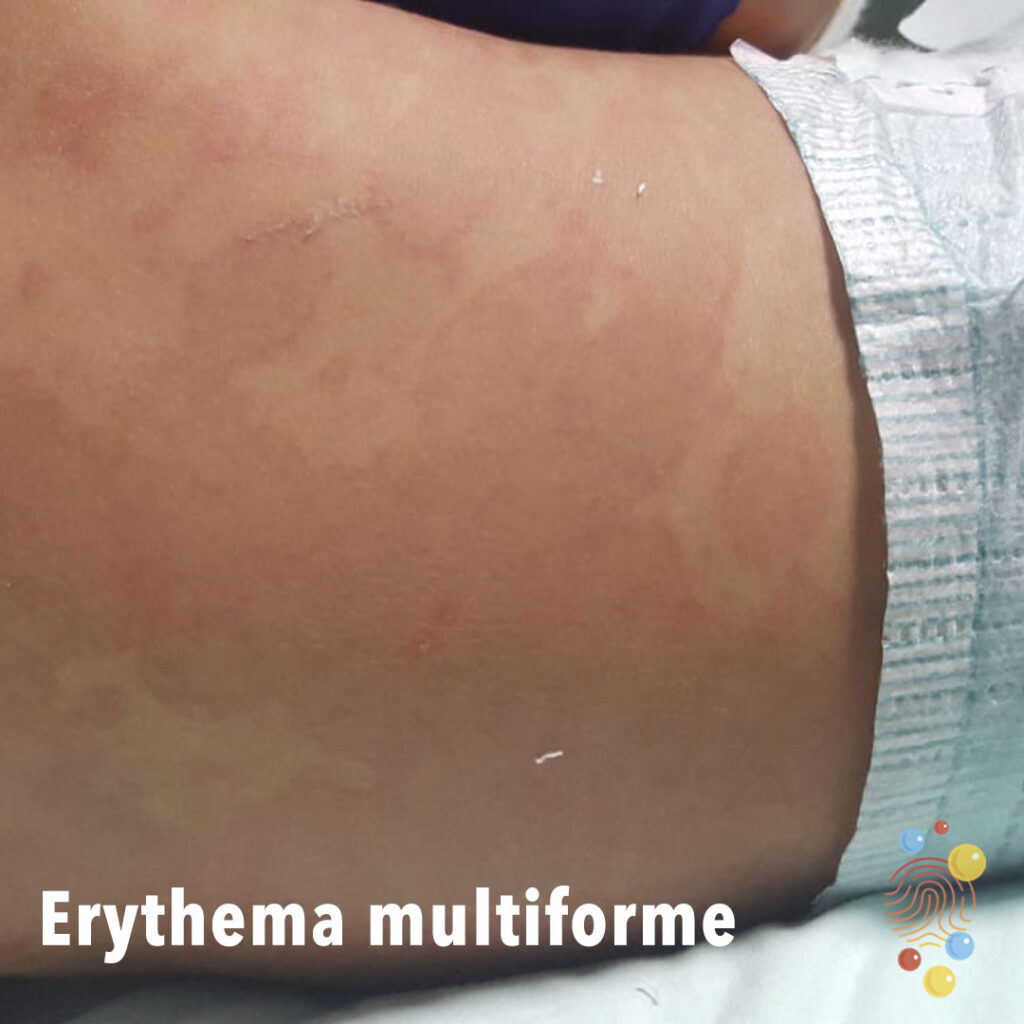
Cutaneous EM lesions arise abruptly and usually in a symmetric, acral distribution on extensor surfaces of extremities (hands, feet, elbows, knees), face and neck. They often appear peripherally (acrally) then spread centripetally. The lesion periphery is usually erythematous and oedematous while the centre becomes violaceous and dark, i.e. a target lesion.
Mucosal lesions are present in up to 70% of patients, favouring oral mucosa. Eye involvement (pain, bilateral conjunctivitis) and urogenital lesions may also occur.
Prodromal symptoms are uncommon (one-third cases) in most cases however can present as mild upper respiratory tract infection (e.g. cough, rhinitis, fever).
Clinically, a link with herpes (HSV-1 usually, but also HSV-2) can be found in one-half of cases. EM lesions begin on average 7 days after a recurrence of symptomatic or asymptomatic herpes.
M.pneumoniae is the next most common cause of EM, especially in paediatric cases. These cases may present with clinical signs (cough, tachypnoea, hypoxia) and radiology of atypical pneumonia.
Diagnosis
EM may be suspected based on clinical features. A skin biopsy and laboratory investigations (direct immunofluorescence, serum antibodies) are useful if the diagnosis is uncertain.
Differential diagnosis:
- Urticaria
- Adverse drug reaction with EM-like features
- Bullous pemphigoid
- Steven-Johnson Syndrome (SJS)
Management
Consider hospitalisation if EM occurs with oral lesions severe enough to impair feeding, when a diagnosis of SJS is suspected, or when constitutional symptoms are present.
General management involves symptomatic treatment with topical steroids, antihistamines and treating the underlying cause. Recurrent EM associated with HSV should be treated with prophylactic antiviral therapy.
References
Paller, A., Gilchrest, B. A., Katz, S. I., Leffell, D. J., Wolff, K., Goldsmith, L. A. (2012). Fitzpatrick’s Dermatology in General Medicine, Eighth Edition, 2 Volume Set. United States: McGraw-Hill Education.
King, C., 2022. Erythema multiforme – DermNet. [online] Dermnetnz.org. [Accessed 3 January 2023].