Background
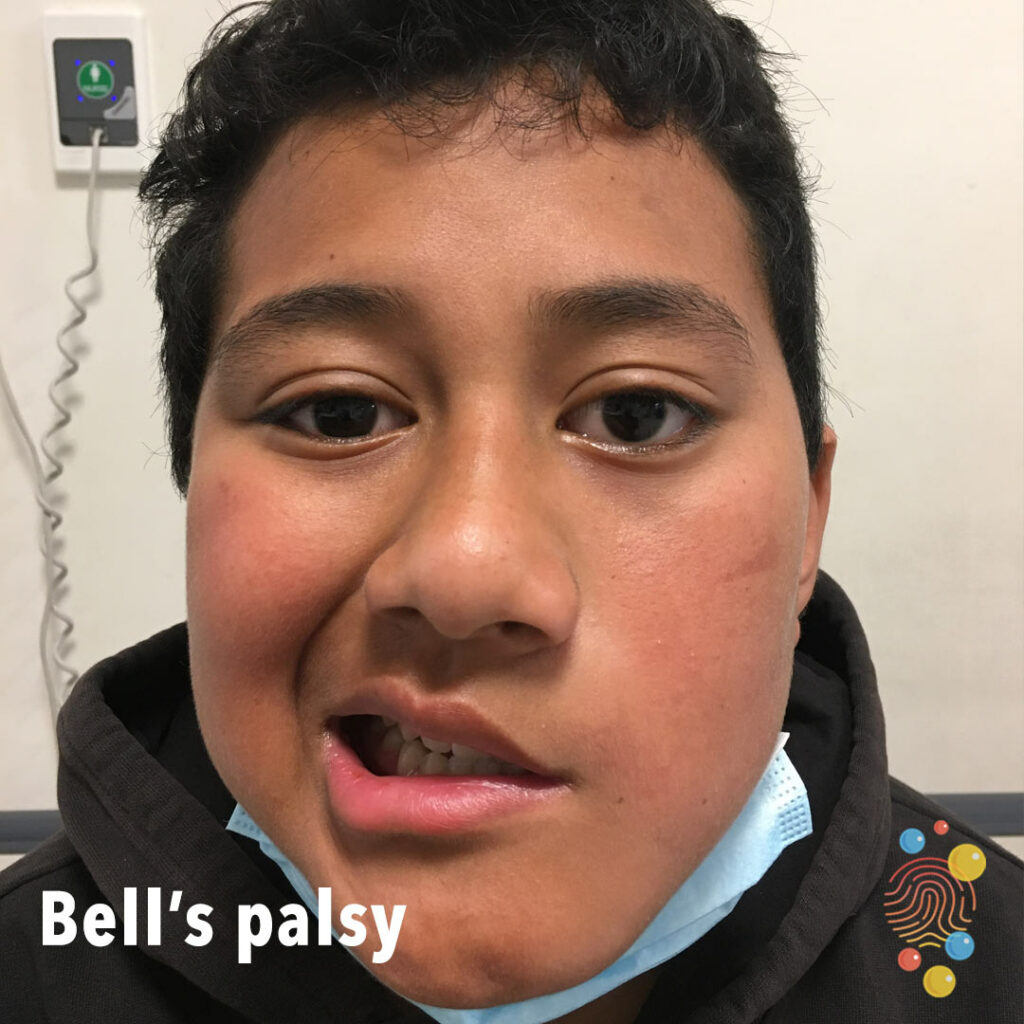
Bell’s Palsy is typically an idiopathic, isolated lower motor neuron lesion of the facial nerve. It is the most common cause of facial paralysis in children and complete recovery is expected, without chronic effects.
Signs and Symptoms
History taking should be focused on the following aspects:
- Progression of the weakness
- Precursory viral infections or trauma involving the facial region
- Presence of facial pain
- Cranial nerves exam, with particular focus to the facial nerve
- Ear examination, looking specifically for otitis media
- Increased sensitivity to sound and altered taste
- Skin lesions or blisters proximal to the ears
Diagnosis
Bell’s palsy is a clinical diagnosis: unilateral facial weakness with an onset of 72 hours, with all other major differentials ruled out.
Differentials
There are a number of different causes of facial weakness that must be excluded when considering Bell’s Palsy, such as inflammation, infection, malignancy, vascular events or trauma.
Management
The management of Bell’s Palsy is characterised by three main components:
- Eye care
- As children may not be able to close their eye this is crucial to protect the eye
- Lubricating eye drops and an eye pad are the two components of eye care
- As children may not be able to close their eye this is crucial to protect the eye
- Steroids
- Prednisone may be used in the 72 hour period of Bell’s Palsy presenting.
- Anti-virals
- Aciclovir can be considered if facial rash present
References
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4677084/
https://www.rch.org.au/clinicalguide/guideline_index/Facial_weakness_and_Bells_palsy/