





The BCG vaccine is a live, attenuated strain of Mycobacterium bovis, first used in humans in 1921. There has been a global shortage of the BCG vaccine since 2012 which has resulted in millions of newborns going unvaccinated. The BCG vaccine has about a 50% efficacy which implies that patients with BCG vaccination can still have tuberculosis. BCG is more effective in preventing children from developing disseminated (miliary) TB or TB meningitis.
TB in children often presents in a non-specific way. Symptoms of TB include weight loss or failure to gain weight, fever, night sweats and fatigue. Patients may have persistent or chronic cough and asymmetrical and persistent wheeze caused by airway compression due to enlarged tuberculous peri-hilar nodes.
Sputum and gastric aspirate mycobacterial cultures have a low diagnostic yield since most children have paucibacillary TB (low bacterial load) unless they have lung cavities. . Recently, diagnostic sensibility for these samples has increased due to the rollout of new molecular techniques (GeneXpert TB PCR).
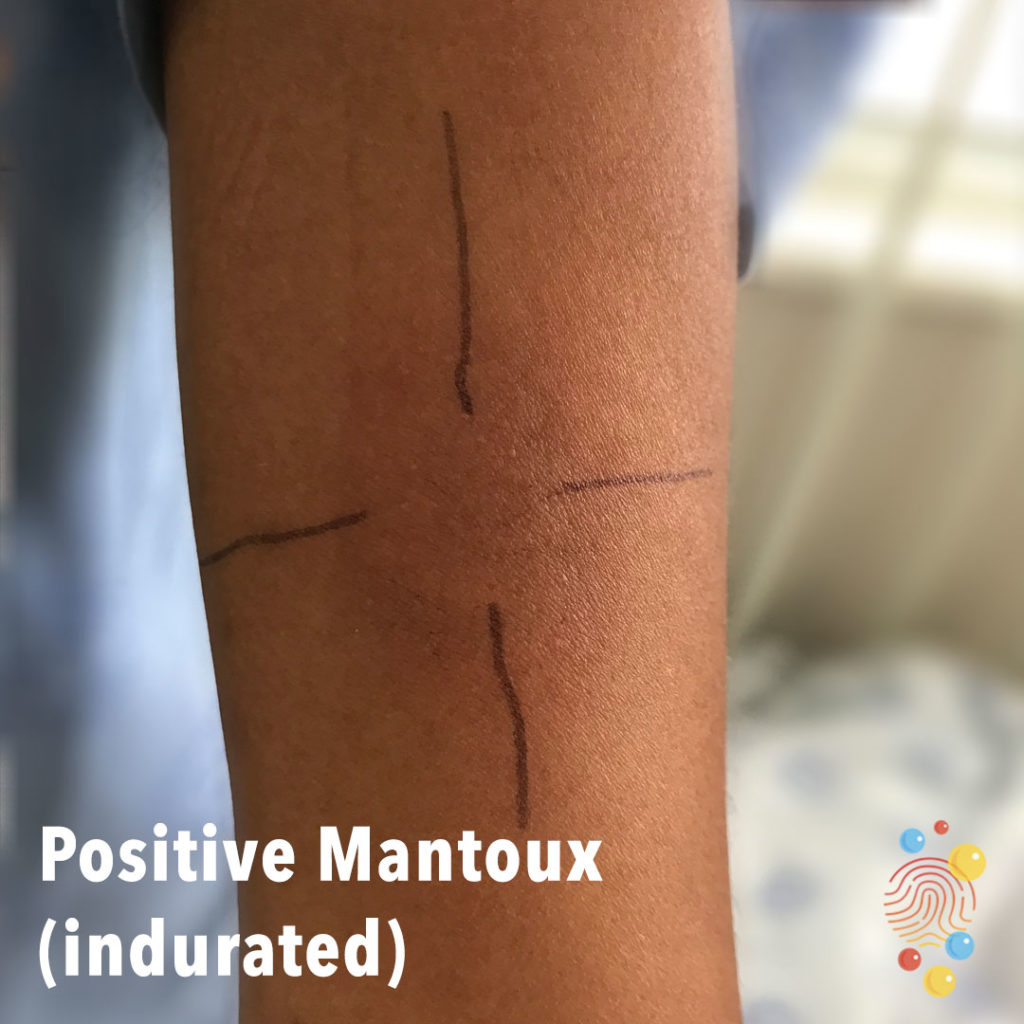
Mantoux test
TST (Mantoux test) and new immunological assays such as IGRAs detect exposure. TST is performed by injecting 0.1ml of tuberculin purified protein derivative (PPD) intradermally into the inner surface of the forearm. The skin reaction produced by the PPD should be read between 48 and 72 hours. The reaction is measured in millimetres of induration, not redness. There are different measures to define a positive result depending on patient background history (for example BCG vaccination) and there are also many causes of false positive and false negative results.
BCG abscess
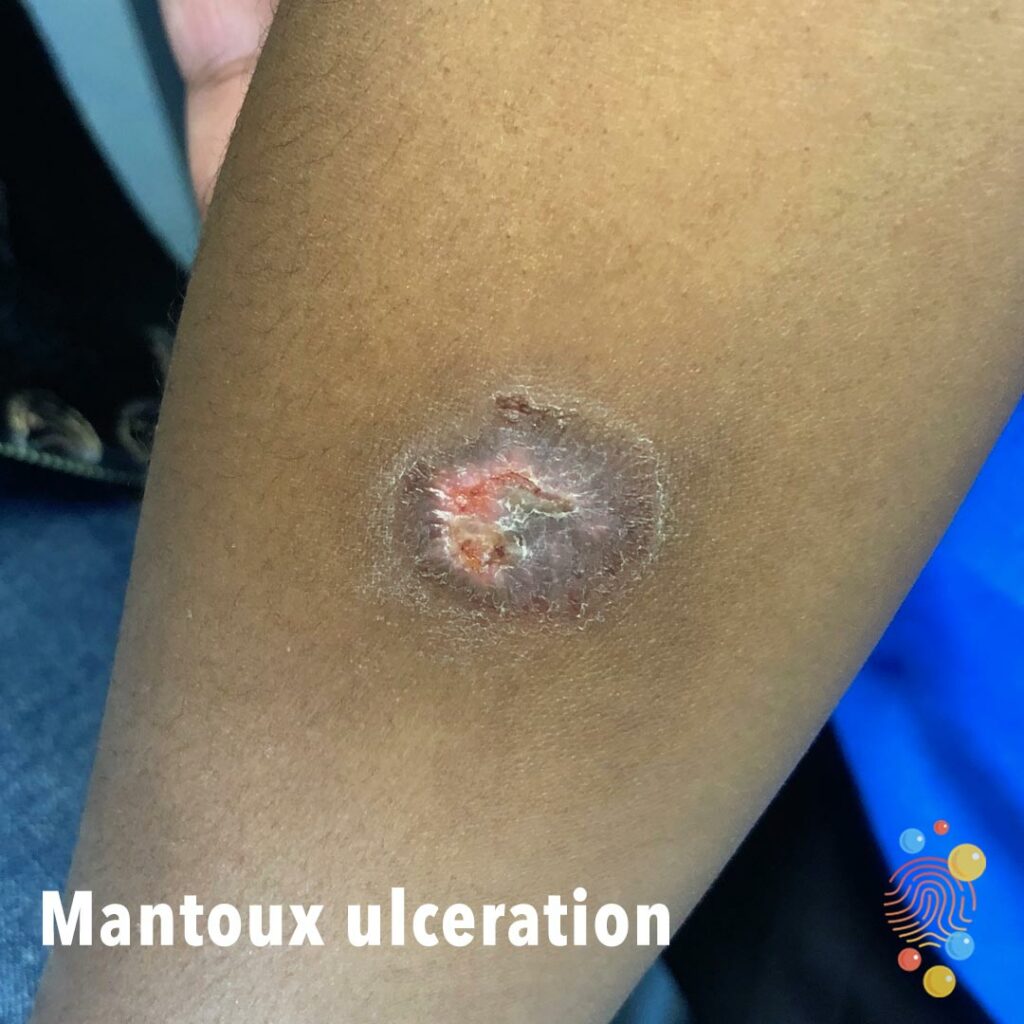
A typical reaction following BCG vaccination is a red, indurated area at the injection site, which may ulcerate 2-3 weeks after vaccination. A crust will then forms after 3-4 weeks. After 6-10 weeks the crust falls off, leaving a small scar. (1,3) Axillary lymphadenopathy (<1cm) is also a normal response to vaccination.
Localised adverse reactions occur in approximately 1 in 1000 people and can include: lymphadenitis, abscesses, persistent injection site reactions and keloid reactions. Systemic adverse reactions are rare and include osteomyelitis and disseminated BCG disease. (1) Systemic disease is usually only seen in children with immunodeficiency or HIV.
BCG abscesses usually present between one and five months after vaccination.
The optimal treatment of BCG abscess is controversial. Options include watchful waiting, antibiotics, needle aspiration and surgical excision.
Isoniazid, rifampicin and erythromycin have all been used to treat BCG abscess but the evidence for their use is limited.
If treatment is required needle aspiration is preferable to incision and drainage because it reduces the risk of developing a draining sinus. Surgical excision should only be performed when needle aspiration has failed.
References
https://www.cdc.gov/tb/publications/factsheets/testing/skintesting.htm
https://dontforgetthebubbles.com/tuberculosis/
https://en.wikipedia.org/wiki/BCG_vaccine
Venkataraman A, Yusuff M, Liebeschuetz S, Riddell A, Prendergast AJ. Management and outcome of Bacille Calmette-Guérin vaccine adverse reactions. Vaccine [Internet]. 2015 Oct 5 [cited 2020 Aug 20];33(41):5470–4. Available from: /pmc/articles/PMC4582770/?report=abstract
Health AGD of. Adverse events following immunisation with BCG vaccination: baseline data to inform monitoring in Australia following introduction of new unregistered BCG vaccine. [cited 2020 Aug 20]; Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cda-cdi4004d.htm
Riordan A, Cole T, Broomfield C. Fifteen-minute consultation: Bacillus Calmette-Guérin abscess and lymphadenitis. [cited 2020 Aug 20]; Available from: https://bestbets.org/bets/bet.php?
Ayazi P, Mahyar A, Taremiha A, Ghorani N, Esmailzadehha N. Effect of oral cephalexin in the treatment of BCG lymphadenitis Effetti di cefalexina orale per il trattamento della linfadentite da BCG.
BestBets: Is medical therapy effective in the treatment of BCG abscesses?
https://journals.lww.com/pidj/Fulltext/2021/11000/Management_of_Bacille_Calmette_Gu_rin.24.aspx