
Introduction
Eye trauma is a common presentation to the Paediatric Emergency Department (PED), with corneal abrasions representing almost half of these.
A corneal abrasion is a scratch to the cornea, the clear, dome-shaped surface that covers the front of the eye. Children with corneal abrasions typically present with a history of trauma and symptoms of foreign body sensation. The commonest cause is direct minor trauma such as tree branches or twigs, pebbles, a fingernail or toys. Sand and other small particles can also cause a corneal abrasion, especially if the child has rubbed their eyes.
Symptoms
The commonest symptoms associated with corneal abrasion are:
- Redness in the affected eye
- Pain particularly when the child looks at a light
- Tearing (watering) of that eye
- Foreign body sensation
- Excessive blinking in the affected eye
- Decreased visual acuity
History
Most cases will be associated with direct trauma. When assessing a painful eye, the following questions should be asked:
- Onset and duration
- Previous ocular history
- Do they wear contact lenses or glasses and if there was prolonged contact lenses use
- Symptoms: pain, foreign body sensation, visual disturbance, either temporary or persisting, including flashes (retinal detachment) or floaters (intra-ocular) in vision , diplopia, lacrimation, photophobia or discharge
- Proximity to chemicals or high velocity projectiles (particularly lawn-mowers, power tools, hammering or motor vehicle accidents)
Examination
Corneal abrasion can be very painful. It’s worth considering administering local anaesthetic eye-drops prior to attempting a thorough examination of the child’s eye.
The eye exam itself should begin by using a pen torch to look for obvious surface abnormalities of the eye and surrounding tissues. Before fluorescein staining look for pupillary light reflex, pupil shape and size, presence of hyphema or hypopyon or a cloudy cornea (prior to blood settling). The presence of hyphema or hypopyon requires an immediate ophthalmologic referral, as do significant decreases in visual acuty.
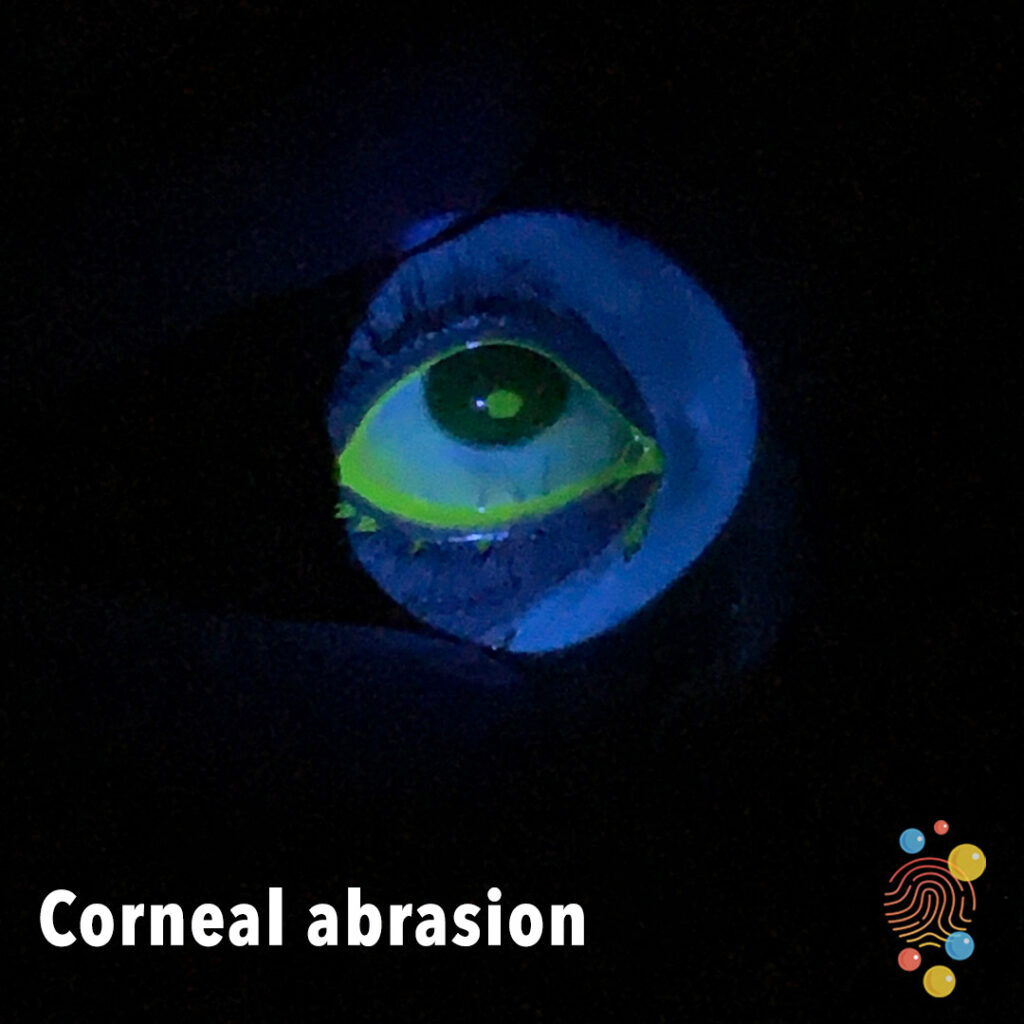
Staining the eye with fluorescein and viewing under a coloured (cobalt blue or green) light from an ophthalmoscope can highlight conjunctival defects or corneal epithelial defects, and makes abrasions easier to see. Don’t forget to look under the eyelid for foreign bodies. Vertically-linear corneal abrasions are particularly suggestive of this.
Management
The mainstay of treatment involves appropriate analgesia and prophylaxis against infection. Most corneal abrasions heal regardless of therapy in 1 to 3 days, with topical antibiotics helping to prevent infection. In high-risk cases, it may also be worth considering a tetanus booster vaccine.
Oral analgesia such as paracetamol or ibuprofen should be used for pain relief. Patching was previously routine but is no longer recommended for most children as patches do not improve the rate of abrasion recovery or reduce pain. Contact lenses should not be worn while the corneal abrasion is healing. Cycloplegic eye drops (cyclopentolate 1%) can be used for relief of a very painful eye.
There are several antibiotic options. Ointment formulations, such as chloramphenicol 1%, provide lubrication to the injured eye. Ointment has the additional benefit of coating the eye with a thin protective film but it can be difficult for some parents and they often find drops easier to administer. Contact lens wearers will need additional antibiotic prophylaxis for pseudomonas with a fluoroquinolone or aminoglycoside.
Topical corticosteroids should never be used due to delayed healing and increased risk of infection. It is important to remind the child not to rub his or her eyes as this can make the abrasion worse.
Complications
Complications associated with corneal abrasions include corneal ulcers, bacterial keratitis, recurrent erosion syndrome, and traumatic iritis.
Corneal abrasions that have not healed after 3 to 4 days, or children who are unwilling to open the affected eye after 24 hours will require urgent referral to an ophthalmologist.
References
Rittichier, K, Roback, MG, Bassett, KE, 2000. Are Signs and Symptoms Associated With Persistent Corneal Abrasions in Children? Archives of Pediatrics & Adolescent Medicine. 154 (4) 370-374.
Browner, EA, 2012. Corneal Abrasions. Pediatrics in Review. 33 (6) 285-286
Ghadah S. Al-Saleh, Alfawaz, AM, 2018. Management of traumatic corneal abrasion by a sample of practicing ophthalmologists in Saudi Arabia. Saudi Journal of Opthalmology. 32 (2) 105-109.
Elghonemy, A, 2017. Patching in Corneal Abrasions in Children. Journal of Opthalmology and Related Sciences. 1 (1) 39-43.
Wippweman, JL, Dorsch, JN. 2013. Evaluation and Management of Corneal Abrasions. American Family Physician. 15; 87 (2) 114-120.